
The funny bone is neither funny nor a bone. The source of pain when someone “hits their funny bone” is actually related to a nerve on the inside of the elbow. This nerve is called the ulnar nerve. The ulnar nerve is one of the three important nerves which control the hand. It supplies feeling to the pinky and ring finger. It also controls many of the fine motor skill muscles in the hand. When the ulnar nerve is not working properly, the pinky and ring finger go numb and tingly and the hand can become weak and uncoordinated. Pins and needles, electric pain, and hand numbness are all very common. This is what happens when the ulnar nerve “funny bone” is hit too hard at the elbow.
Cubital tunnel syndrome
Cubital tunnel syndrome is a common type of pinched nerve, and is related to the ulnar nerve at the elbow. This is the same nerve involved when a person hits their “funny bone.” Patients may experience symptoms such as numbness, tingling, weakness, and pain in the hand and forearm.
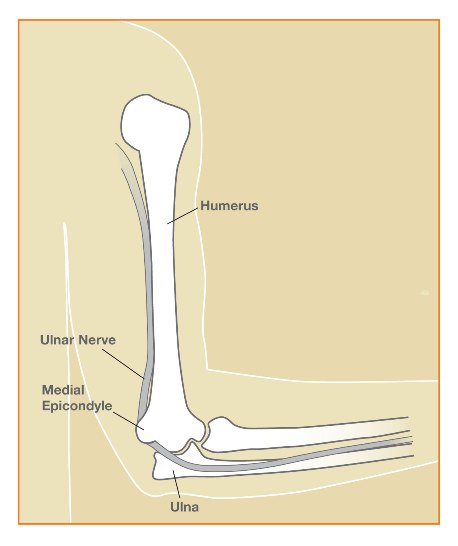
As the ulnar nerve travels from the upper arm into the forearm, it courses through the normal groove behind the bony bump on the inside of the elbow (the medial epicondyle). The ulnar nerve is at risk for compression at this site – within the cubital tunnel – as it turns the corner around the elbow. In this area of the elbow, the ulnar nerve is pretty close to the skin and can be bumped easily. The nerve then travels down the forearm and innervates muscles in the forearm and hand and provides sensation to the small finger and ring finger. It is thought that pressure on the nerve reduces neural blood flow, causing symptoms in the hand.
How do I know if I have cubital tunnel syndrome?
Patients with cubital tunnel syndrome usually report numbness and tingling in the pinky and ring fingers, or a feeling that these fingers are asleep or swollen. Some people feel “electric” or “shooting” pain down the forearm into the hand, similar to the feeling of “hitting the funny bone”.
Some patients report increased symptoms when the elbow is bent (flexed), such as while talking on a cell phone, driving, or sleeping. Dropping objects, clumsiness with the hands, or a weak grip are also common complaints. In severe or long-standing cases, the small muscles within the hand can become weak and atrophy. This can lead to permanent deformity of the hand, weakness, and hand dysfunction.
Often the diagnosis can be made on the basis of patients symptoms, medical history, and physical examination in the office. Hand surgeons are experts in diagnosing nerve conditions in the hand and arm. A nerve conduction study can confirm the diagnosis and assess the severity of the nerve compression.
Not all hand pain or numbness is caused by cubital tunnel syndrome or ulnar nerve problems. Nerves in the arm can be compressed or “pinched” anywhere along their pathway from the neck to the fingers. Therefore it is important to identify the location of the nerve compression.
What are the treatment options?
Non-operative treatment is usually tried first as symptoms can be relieved without surgery in many cases. Wearing an elbow splint during sleep prevents the elbow from flexing too much. This can be prescribed in clinic or made at home with a rolled towel or pillow to keep the elbow straight. Avoidance of prolonged and repetitive elbow flexion, pressure on the inside of the elbow, and vibratory tools may reduce symptoms. Wearing an elbow pad during activities can reduce the pressure on the nerve. Hand therapy can be done, including nerve gliding exercises. Medications are occasionally prescribed if the nerve pain is severe.
If these measures fail to improve the condition, or if the nerve compression is severe, surgery may be recommended. There are several types of procedures available. The type of procedure performed varies between surgeons and patients, but the most important factor is releasing all the sites of pressure on the nerve. Two of the most commonly performed procedures are described below:
Ulnar nerve decompression surgery: The least invasive procedure is known as a cubital tunnel release. This procedure decreases pressure on the ulnar nerve by removing tight bands of tissue on the nerve. There are several sites within the elbow where the nerve can be pinched, and each of these areas are evaluated and treated during surgery.
Ulnar nerve transposition surgery: An ulnar nerve transposition decreases pressure and tension on the ulnar nerve by shifting the nerve’s course around the elbow. During transposition surgery, the ulnar nerve is moved out of its groove behind the elbow to the front of the elbow. At the conclusion of the procedure, the nerve is positioned in a bed of tissue either under the skin, within muscles, or beneath muscles of the forearm.
What is the recovery from surgery?
These surgeries are performed as an outpatient usually with nerve block anesthesia. Patients may use their hands for light activities starting the day after surgery. Most people can return to light duty work after a few days. In most patients, a soft bandage is used to cover the incision and gentle elbow range of motion is allowed. A plaster splint is used if a “transposition” procedure is performed. Avoiding forceful lifting, pulling, pushing or gripping for approximately 4 weeks after surgery is usually recommended.
What are the results from surgery?
Most patients report decreased numbness, tingling, and nerve pain in the hand after surgery. Recovery of the ulnar nerve after surgery is usually slow, and nerve recovery can take several months. Some patients do not regain full strength or normal sensation in the hand, especially in severe or long-standing cases. Mild soreness and numbness at the incision site often improves over a few months.
What are the complications from surgery?
Major complications from cubital tunnel release are uncommon. Possible complications include persistent symptoms, bleeding, infection, elbow stiffness, and damage to the nerves. A skin nerve at the incision site can become irritated in some patients.
Disclaimer: Please note, the material provided on this site is intended for general information only and does not constitute medical advice. This does not replace evaluation by a doctor. Please seek medical evaluation if you have a concern.