Carpal tunnel release surgery is one of the most common procedures performed in the United States. Over 90% of patients are pleased with the results, and they would recommend the surgery to a loved one. Most patients have decreased hand numbness, no night-time hand tingling, and less pins and needles hand pain. Many of my patients tell me that after surgery they were able to sleep well for the first time in months.
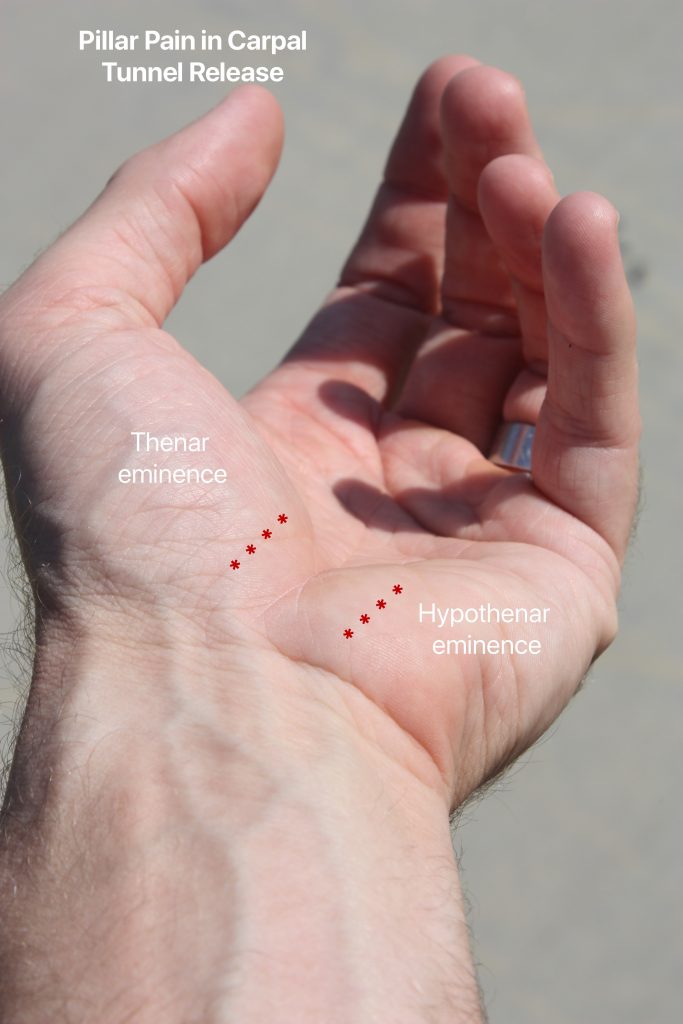
However, surgical site pain can be a temporary problem for some patients. “Pillar pain” is a frequent symptom following carpal tunnel release. The pain is located at the base of the hand in the palm, within the muscles at the thumb base (thenar eminence) and the muscles at the base of the small finger (hypothenar eminence). The palm is tender when pressed in these areas (marked with red asterisks in photo). This condition can occur with either open carpal tunnel release or endoscopic carpal tunnel release, but is more common in open surgery.
Most patients can return to office work within a week and heavy manual labor within 3-4 weeks following carpal tunnel release. Pillar pain can make recovery from carpal tunnel release surgery take longer than expected. Putting pressure on the palm, such as trying to do a push-up or gripping a golf club, can increase the soreness.
Pillar pain does not last forever. The symptoms go away within 3 months in most patients. Occasionally pillar pain can last 6 months. The vast majority of patients no longer have this type of pain 12 months after surgery.
There is not a good way to predict who will get pillar pain with surgery. No one knows why pillar pain occurs. There are several theories to explain this condition:
Tender scar tissue: There are bony prominences in the palm in the locations of pillar pain. Inflamed scar tissue from surgery can be tender overlying these bones. The trapezium bone (within the thenar eminence) and the hamate bone (within the hypothenar eminence) are both close to the skin in the palm.
Changes to muscle alignment: When the transverse carpal ligament is cut, there are subtle changes to the mechanics of the carpal bones and the palmar muscles. This might contribute to pillar pain.
Joint inflammation: Additionally, inflammation within the nearby joints can cause pain. The thumb carpometacarpal (CMC) joint is a common site of wear and tear arthritis. If this joint had previous arthritis, it can become inflamed and painful within the thenar eminence. This process can also occur at the hypothenar eminence within the piso-triquetral joint.
Nerve irritation: There are many skin sensory nerve branches in the hand and palm. These nerves might be irritated from the surgical dissection and healing scar tissue.
Treatment of pillar pain usually helps to improve the symptoms. Hand therapy is sometimes recommended. Stretches, nerve gliding exercises, scar massage, splinting, iontophoresis, and other modalities can be used by hand therapists to reduce pain. Steroid injections are occasionally used to reduce scar tissue formation as well. Revision surgery is not necessary for this condition. Most patients do not require oral medications for pillar pain.
I tell my patients to keep using their hands while working through the pain. After the carpal tunnel incision has healed, hand activity is not harmful to the recovery process. Doing too much with the hands after surgery can be sore, but it does not cause long-lasting damage. Eventually, pillar pain gets better with time.