
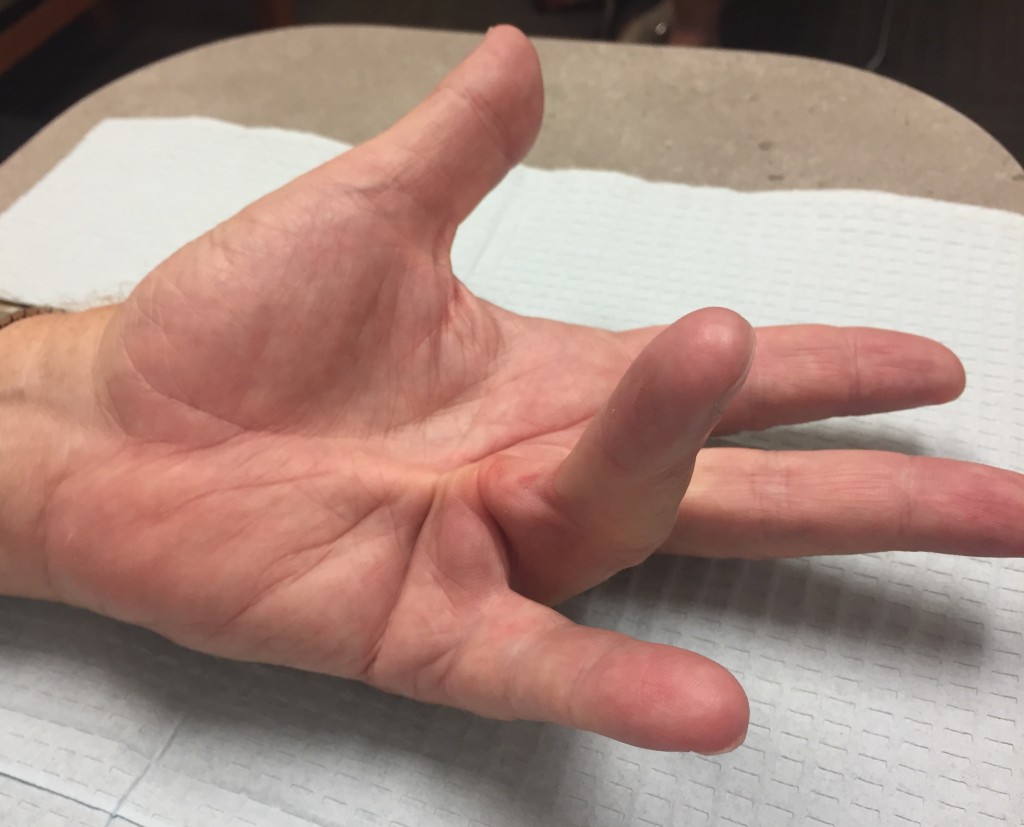
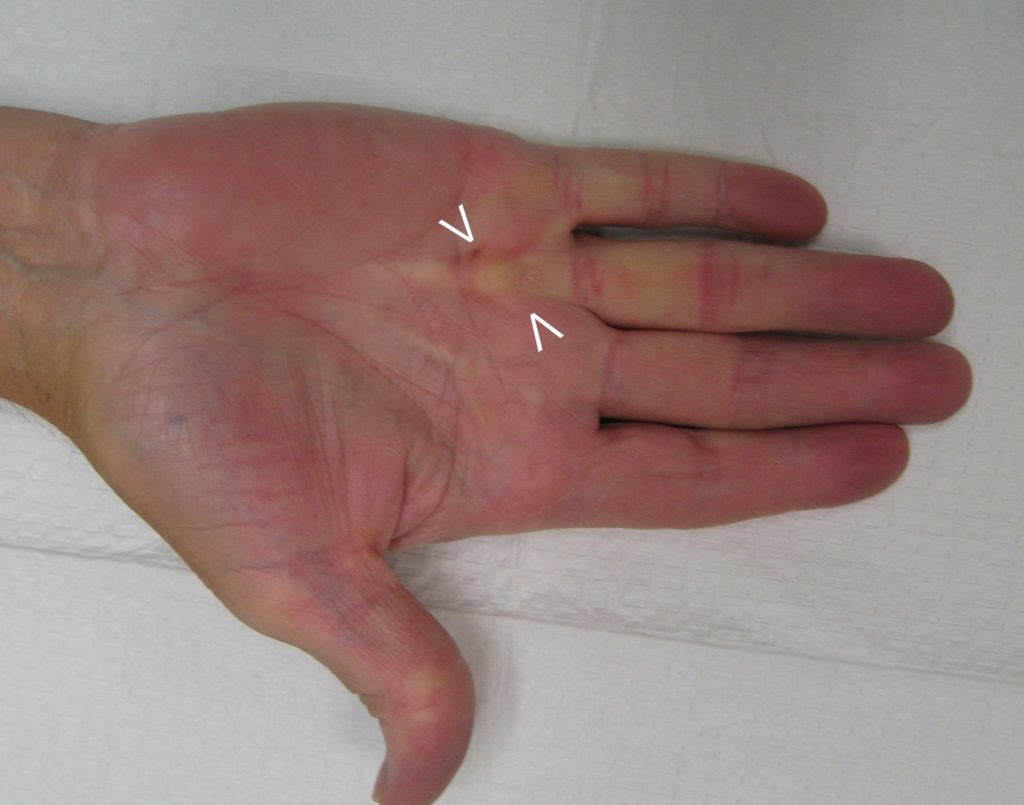
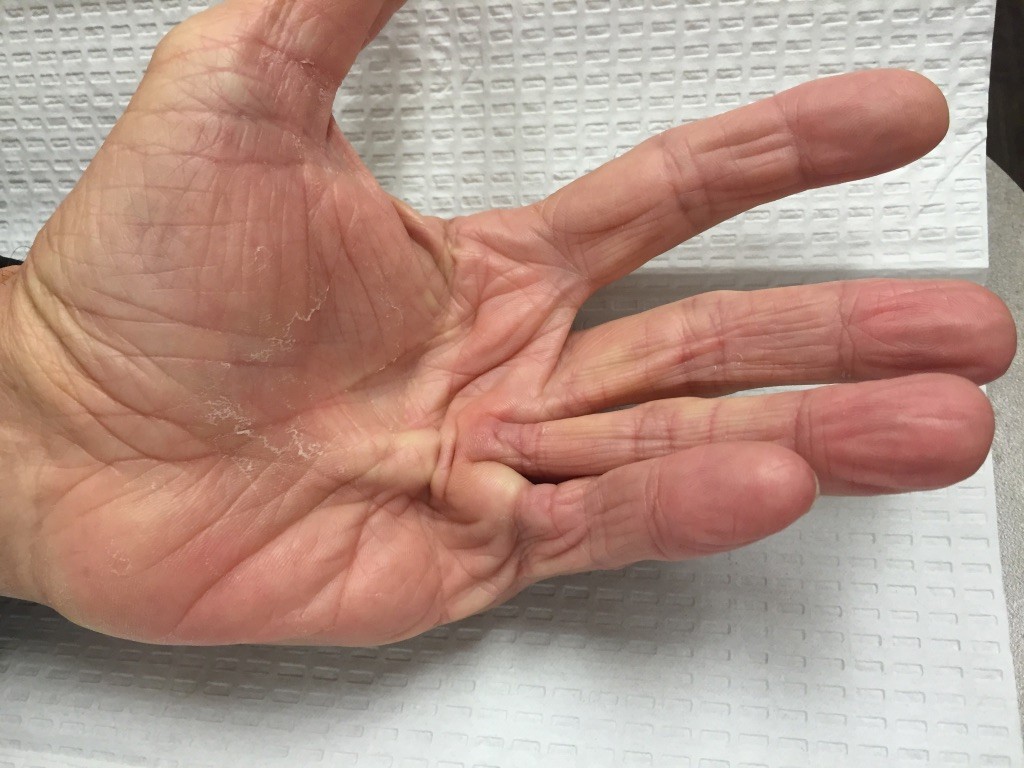
Dupuytren’s disease is a common condition affecting the hand. This condition is characterized by abnormal fibrous tissue formation in the palms and fingers. Early in the course of the disease process, nodules of fibrous tissue develop in the palm. In about a 30-50% of patients, these nodules develop into cords which gradually bend the fingers into a flexed position. Over time, the finger joints become stiff and more difficult to straighten. This is called a flexion contracture. Severe flexion contractures in the fingers can develop which significantly impair the use of the hand. Read below about nonsurgical treatment of Dupuytrens contracture which are available for patients.
Doctors have known about Dupuytren’s disease for several centuries. The condition is named after Guillamme Dupuytren who was a French surgeon in the 1800s. Prior to that, in the 1500s a family of bagpipers in Scotland had a high incidence of this hand condition, and then it was called “MacCrimmon’s curse.” Dupuytren’s has also been called “Viking’s Disease” because it is more common in people with Scandinavian ancestry. Research into this condition has increased significantly over the past several years. However, there is still much to be learned about Dupuytren’s disease.
Risk factors for Dupuytren’s disease include male sex, family history of the condition, Northern European ancestry, smoking, alcohol abuse, diabetes, and possibly hand trauma. Patients with Dupuytren’s disease are also prone to plantar fibromatosis (Lederhosen), penile fibrosis (Peyronies), and adhesive capsulitis (frozen shoulder).
Treatment Of Dupuytrens Nodules
Treatment options are available for patients with Dupuytren’s at various stages of the disease. Currently, there are no cures for Dupuytren’s and no proven way to slow down the disease process. Corticosteroid injections (cortisone shots) are sometimes used to reduce pain, itching, or discomfort from Dupuytren’s nodules in the palm. Steroid injections can shrink and soften the nodules in most patients, however, the nodules often come back in the future. Topical medications such as verapamil, Vitamin E, and steroid creams are being studied for treatment of palmar nodules. Radiation treatment is considered controversial for Dupuytren’s disease. Radiation is used more commonly in Europe compared to practices in the United States.
When a joint contracture has developed from a Dupuytren’s cord, there are two non-surgical treatments for patients with Dupuytren’s contracture: needle aponeurotomy and collagenase injections. Both procedures are performed in the office. These procedures can significantly improve finger range of motion and patients have a much quicker recovery compared to surgery. Patient satisfaction is usually high for these procedures. Not all patients are candidates for these procedures.
Needle Aponeurotomy
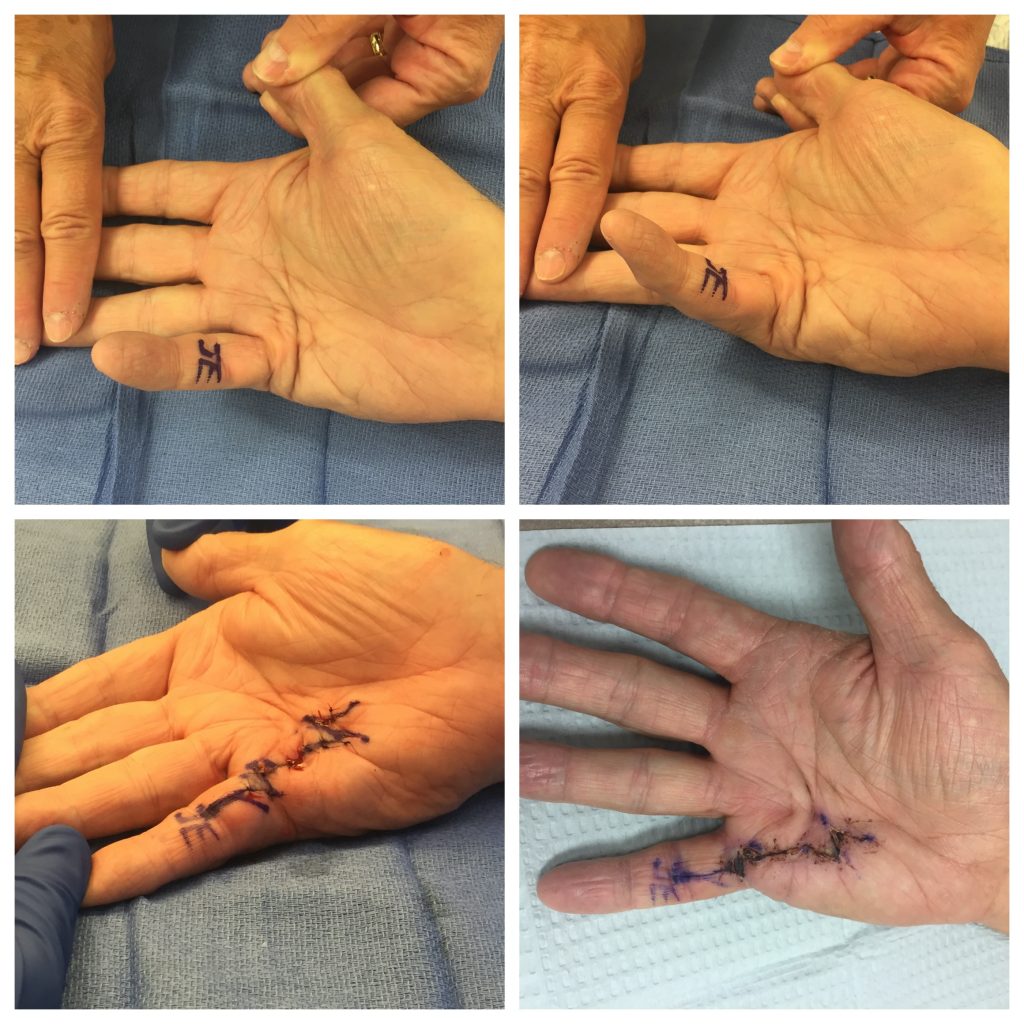
Needle Aponeurotomy (NA) is a minimally-invasive procedure performed under local anesthesia in the office. After injecting numbing medicine, the surgeon uses the tip of a needle to perforate the palpable cords multiple times. Then the fingers are manipulated to rupture the weakened cords, allowing the fingers to straighten. This procedure has some risks: skin tears, pain, bruising, and swelling at the needle site are common. These symptoms usually resolve in a few days. More severe complications such as infections, injuries to the nerves and flexor tendons are very rare. This is the least expensive treatment intervention for Dupuytren’s contracture and the procedure has minimal recovery time. Recurrence rates are high, but the procedure can be repeated in the future for recurrent contractures. This is a “high value” procedure: low cost and high quality.

Collagenase Injections
Another nonsurgical treatment for Dupuytrens contracture is collagenase. Collagenase injections (Xiaflex) were FDA approved for use in the United States in 2010. This minimally-invasive procedure involves an injection of an enzyme to dissolve the palpable Dupuytren’s cords. The injection is performed in the clinic by the hand surgeon. 2-3 days later, the patient returns to the office for a manipulation procedure. This is performed with local anesthesia numbing medicine, and the surgeon gently straightens the fingers to rupture the weakened cords. Similar to NA, collagenase injections are not risk-free. Bruising, pain, and swelling of the hand and lymph nodes is common. Blisters and skin tears can also occur, but these usually heal on their own in a few days. Ruptures of the flexor tendons of the finger are rare (less than 1% of patients), but if this happens, it is a major complication. Allergic reactions to the medication are rare but also possible. Xiaflex collagenase medication is expensive, but it is often covered by many insurance plans. Recurrence rates are high, but the procedure can be repeated in the future for recurrent contractures.
Dupuytrens Surgery
Surgery is the tried-and-true treatment for Dupuytrens contractures in the fingers. Surgery can be performed safely in the operating room to improve finger range of motion and quality of life when patients are not candidates for the non-surgical options. Make an appointment with a hand specialist to learn more about Dupuytren’s. He will discuss if nonsurgical treatment of Dupuytrens contracture is recommended for your case or if surgery is recommended based on your particular condition. Dr. John Erickson is a hand specialist and orthopedic surgeon at Raleigh Hand to Shoulder Center.
Disclaimer: Please note, the material provided on this site is intended for general information only and does not constitute medical advice. This does not replace evaluation by a doctor. Please seek medical evaluation if you have a concern.