
Tumors of the hand and upper extremity are surprisingly common. They can occur in people of all ages — from children to the elderly. Fortunately, the vast majority of these tumors are benign, NOT cancerous. Nevertheless, every tumor should be carefully evaluated. Benign tumors which do not cause pain, dysfunction, or problems do not require surgery. In many cases the treatment involves observation. Occasionally, however, the diagnosis is uncertain, and a biopsy is recommended. Please note that only a trained physician can determine whether a mass is benign or more worrisome.
Ganglion cyst

A ganglion cyst is the most common bump to arise in the hand. Ganglions typically arise near a joint or tendon in the hand and wrist. They are filled with thick, jelly-like fluid, which is thought to be related to the synovial fluid of joints or tendon sheaths. Classically, ganglion cysts are soft, rubbery, and round, but they can be more firm and lobulated in some cases. The most common location is the back of the wrist (dorsal carpal ganglion). These cysts are benign, usually painless, and may fluctuate in size. Some ganglion cysts may disappear without treatment. They are more common in young women, and may be seen in teenagers. For symptomatic ganglion cysts, aspiration with a needle or surgical excision may be offered.
Mucous cyst

A mucous cyst is a specific type of ganglion cyst in the finger. Mucous cysts are benign. These cysts arise from the end knuckle of the finger, the distal interphalangeal (DIP) joint, near the fingernail. They are commonly seen in both men and women 50-70 years of age who have hand arthritis. Bone spurs (also called “osteophytes”) are a sign of arthritis seen on x-rays. Mucous cysts are filled with a clear, thick, jelly-like fluid which is thought to arise from the DIP joint. Occasionally a ridge in the fingernail develops, which is caused by pressure on the root of the nail from the cyst. These cysts can fluctuate in size, and may go away on their own in some cases. Most of the time they are painless, but they can become painful after an injury to the fingertip. Surgery is often recommended to excise the cyst and the root of the cyst within the joint.
Epidermal inclusion cyst
Inclusion cysts are thought to be related to implantation of skin (epidermal) cells within the underlying soft tissues of the hand after a puncture or traumatic wound. Most people recall a penetrating injury to the skin before the mass arises, however, some do not. Inclusion cysts are often on the palm-side of the hand and commonly on the fingertip. These masses are benign, slow-growing, firm, round, and often painless. For symptomatic inclusion cysts, surgical excision has a low recurrence rate.
Dupuytren’s nodule
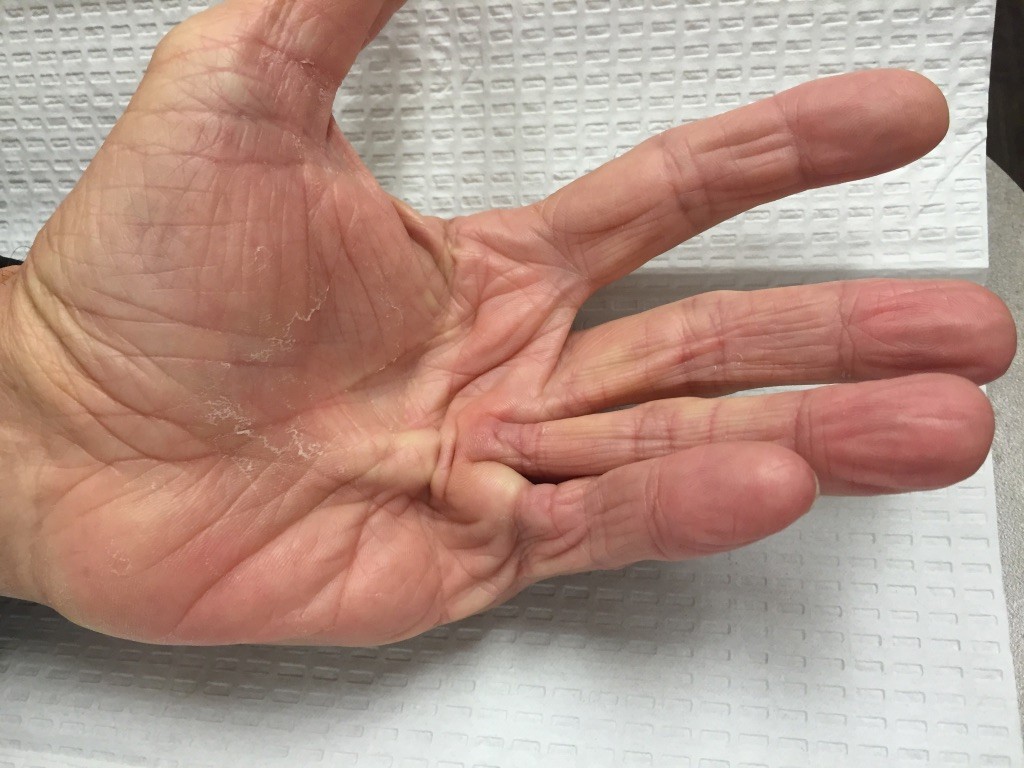
Patients with Dupuytren’s disease may develop a bump in the palm early on in the disease process. These are firm nodules which can be tender to firm pressure such as gripping the steering wheel. The nodules are made of a type of collagen similar to scar tissue. Many patients confuse these nodules with ganglion cysts. Often patients will have these in both palms and have a family history of Dupuytren’s. Patients can get a similar condition in the arches of the feet. Sometimes the disease continues to get worse and the fingers draw in due to Dupuytren’s cords in the palm. When the fingers contract over time, it is difficult to straighten the finger.
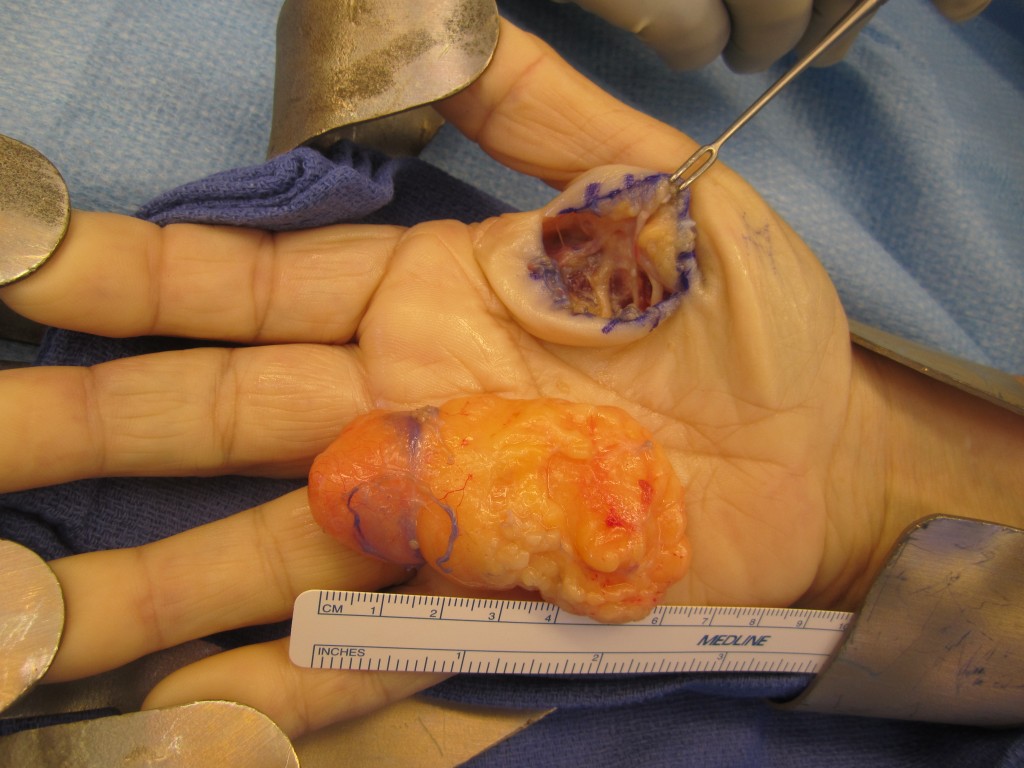
Giant cell tumor of tendon sheath (GCT)

GCT is a benign soft tissue tumor which is common in the upper extremity. Despite the name, the tumor does not always arise from a tendon sheath, but can occur at any location within the hand. The term “giant cell” relates to the appearance of the tumor cells under the microscope. The most common sites are the palm-surfaces of the thumb, index, and middle fingers. The mass is slow-growing, firm, lobulated, and usually painless. These tumors can grow larger if left alone. After surgical excision, recurrence rates can be high, approximately 30% in some studies. GCTs which directly involve a joint or tendon may have a higher recurrence rate. The cause of GCTs is unknown.
Lipoma
A lipoma is a common, benign soft tissue tumor composed of fat cells (lipocytes). Diet and activity level are not related to the cause. These tumors may have been present for years and usually are slow growing. They are often soft, mobile, and easily felt within the soft tissues just beneath the skin (subcutaneous). In most cases they are painless and do not interfere with hand function. Deep or large lipomas may compress adjacent structures, such as nerves. For symptomatic lipomas, surgical excision has a low recurrence rate.
Nerve tumors
Nerve tumors are often benign tumors arising from the nerves of the body. A schwannoma is the most common benign nerve tumor of the upper extremity. These tumors are slow-growing, usually painless, but may cause a neurologic symptom such as weakness or numbness in the hand. In most cases, complete excision of a schwannoma can be performed while preserving the nerve. This is because the nerve arises from the nerve sheath and can be dissected away from the intact nerve. There is a low recurrence rate and a small chance of neurologic deficit with surgery. A neurofibroma is another common nerve tumor of the upper extremity. Unfortunately, neurologic deficits are frequent after surgical excision because the tumor is intertwined with the nerve fibers. In other words, a portion of normal nerve tissue must be removed in order to remove the entire nerve tumor. Nerve grafting may be advised to bridge a nerve defect after neurofibroma excision. Patients with neurofibromatosis disease (NF) have multiple neurofibromas at various sites in the body. There is a risk of malignant (cancerous) transformation of neurofibromas in patients with NF. An uncommon type of nerve tumor, the neurofibrosarcoma, is malignant. These nerve tumors are much less common than schwannomas or neurofibromas.
Vascular tumors
The most common type of vascular tumor is a hemangioma. Hemangiomas are benign tumors of blood vessels and are more common in females, infants and children. If they are located on the skin surface, they are often bright red in color (strawberry hemangioma). Deeper tumors are more bluish in color. In the first year of life, these tumors can grow rapidly. As the child ages, the tumor growth rate decreases, and the hemangioma begins to slowly fade and contract (involute). Treatment is typically non-surgical as most hemangiomas resolve spontaneously over time (70% by 7 years of age)
Glomus Tumor
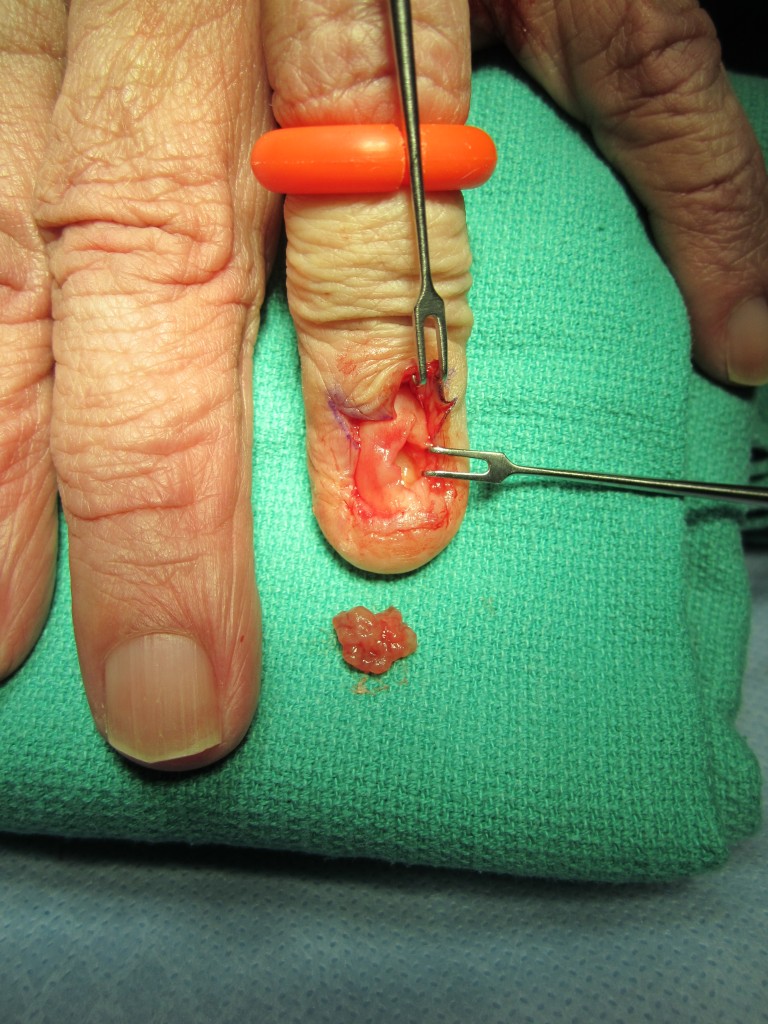
Glomus tumors are benign tumors of the vascular tissue responsible for temperature regulation of the skin and nail bed. These are often small, slow growing tumors which can be very painful. Misdiagnosis is common and the source of pain usually is not identified for several months by physicians. In classic cases, patients report severe, sharp pain exacerbated by cold temperatures and pressure on the area. They are most common in the fingertip, usually under the nail. Surgical excision is frequently successful in pain relief, but recurrence is possible.
Pyogenic Granuloma

A pyogenic granuloma is a benign mass of unknown cause which frequently arises in the hand and upper extremity. These lesions often grow rapidly and appear deep red in color. Pyogenic granulomas may bleed easily with minor trauma as they are rich in blood vessels. They are more frequent in young women, particularly during pregnancy. Treatment includes chemical cauterization with silver nitrate in the office and surgical excision in the operating room. Recurrence after surgery is infrequent.
Skin Tumors and Skin Cancers
Tumors of the skin are very common. Patients typically receive excellent care from primary care physicians and dermatologists for many skin lesions. For larger skin tumors of the hand and upper extremity, referral to a surgeon may be recommended. Squamous cell carcinoma (SCC) is the most common malignancy (cancer) in the hand. Fair skin and excess sun exposure are known risk factors for many skin cancers, including SCC. These tumors grow in size and have the potential to metastasize (spread) to other parts of the body causing disability and possibly death. Surgical excision can be curative if adequate excision of the SCC is performed prior to metastasis. Usually, a margin of normal skin surrounding the tumor needs to be excised in order to ensure complete tumor removal.
Keratoacanthomas are similar in appearance to SCC, but they are thought to have little or no metastatic potential. They typically have a thick keratin crater or core and classically grow rapidly over several weeks. Some keratoacanthomas resolve on their own slowly over 6-12 months, leaving a scar behind. Biopsy can be performed to confirm the diagnosis. Actinic keratosis is referred to as pre-malignant, as these lesions often result in SCC. They often appear as thick, scaly or crusty patches in sun-exposed areas of skin which can increase in size and thickness. Many treatments are available including topical medications, cryosurgery (“freezing”) with liquid nitrogen, and surgical excision.

Basal cell carcinoma (BCC) is another common skin cancer. These tumors may also metastasize, but at a much lower rate than SCC. Excision with a margin of normal, tumor-free skin tissue is recommended. Melanomas are malignant tumors of melanocytes (cells responsible for skin pigmentation).
Melanomas are less common that SCC or BCC, but they are responsible for more deaths due to the aggressive nature of the tumor. Biopsy is usually recommended to confirm the diagnosis and determine the tumor thickness/depth, which guides further treatment. Surgical treatment often includes wide surgical excision and possible lymph node biopsy and lymph node excision. Avoiding prolonged sun exposure and the use of sunblock/protective clothing are important to reducing the risk of skin cancer.
Disclaimer: The information on this website is intended for general information only, and it does not constitute medical advice. This educational material does not replace an evaluation by a qualified medical professional. Please make an appointment with a physician if you have concerns.