“Broken wrists” are a very common type of injury. These fractures frequently occur from a fall at home, a sports injury, or during a car accident. These injuries are very common in children and in older patients with osteoporosis.
The radius and ulna bones are the skeletal foundation of the forearm. At the wrist, the radius is much larger than the ulna and supports about 80% of the force transmitted across the joint. The distal radius is the portion of the radius bone just below the wrist joint, and a fracture of the distal radius is the most common type of broken wrist.
What are the treatment options for a broken wrist?
The treatment plan will depend on the severity of the fracture as noted on the x-rays and the patient’s medical condition, activity level, and desires. The distal radius bone heals back together after a fracture; the main question is whether it will heal in good alignment. In many cases, restoring the function of the hand, wrist and forearm is dependent on satisfactory healing of this injury.
Most people have fractures which are well-aligned, and, therefore, do not require surgery. Treatment in these cases is typically rest and protection in a cast or brace for several weeks. Follow-up x-rays are obtained in clinic to evaluate how the fracture is healing. Children often heal very well from this injury. Most pediatric distal radius fractures can be treated non-operatively due to the potential for the injury to re-align itself during skeletal growth. The process of natural realignment during growth in children is called remodeling.
Some fractures can be re-aligned well without surgery, called “closed reduction”, and those patients can also be treated successfully non-operatively. This is performed either in the office or emergency room using an injection of a local anesthetic (lidocaine). After the bones are “set” a plaster splint is molded to the wrist and forearm to maintain the alignment. Therapy is often helpful in improving wrist range of motion and strength after the fracture heals. It may take several months for strength and range of motion to fully improve.
Some patients have fractures which are more severe and the alignment of the fracture is not satisfactory (“crooked wrist”). Depending on the patient’s health and activity level, surgery may be advised to correct the alignment. In adults, a plate and screws are most commonly used in surgery during a procedure called open reduction and internal fixation (ORIF). In children, temporary pins are most commonly used during a procedure called closed reduction and percutaneous pinning.
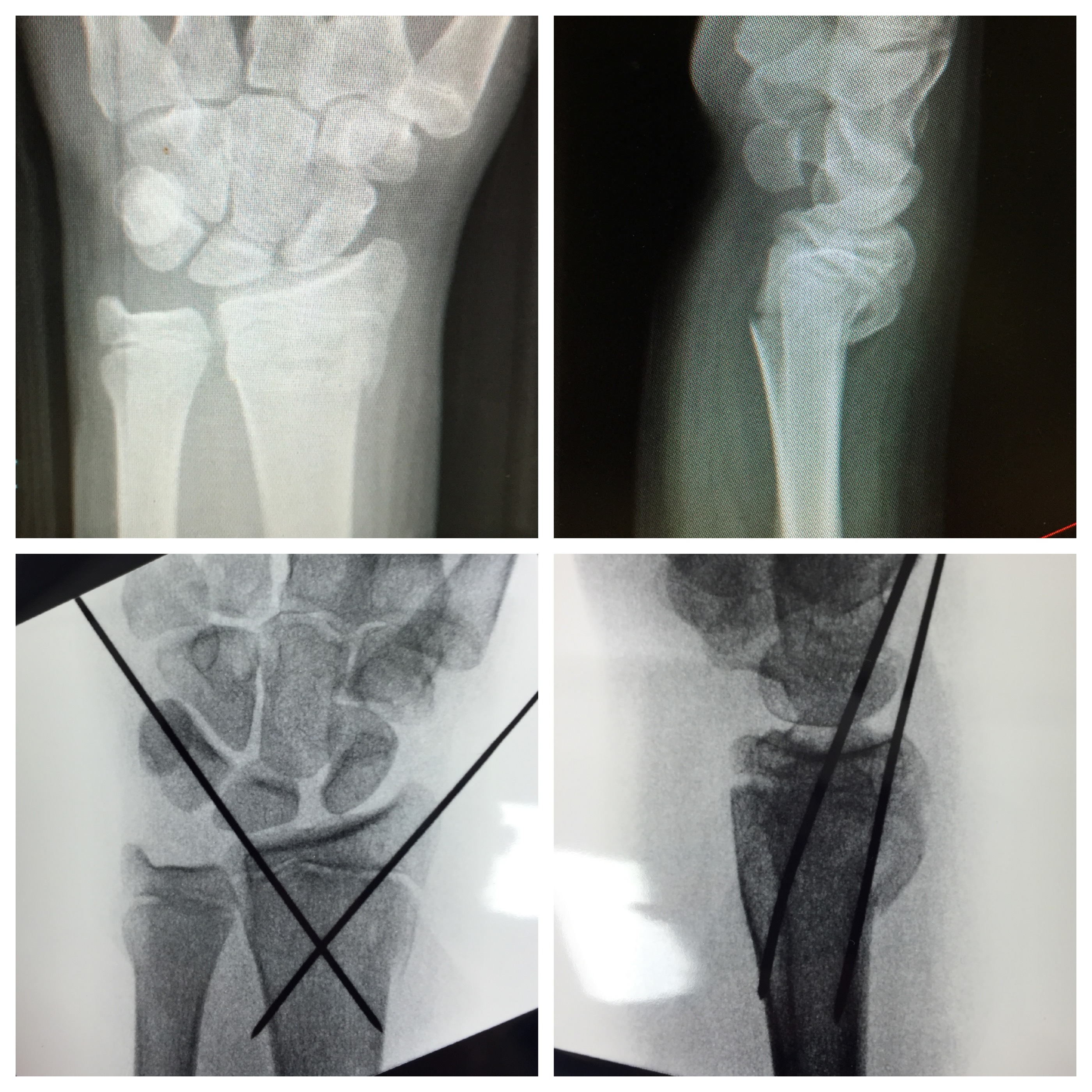
Case #1
The patient in the images below is an adolescent. The child underwent closed reduction and percutaneous pinning due to the unacceptable wrist alignment from the fracture. The pins were kept in place for 4 weeks, at which time the pins were removed in the office.
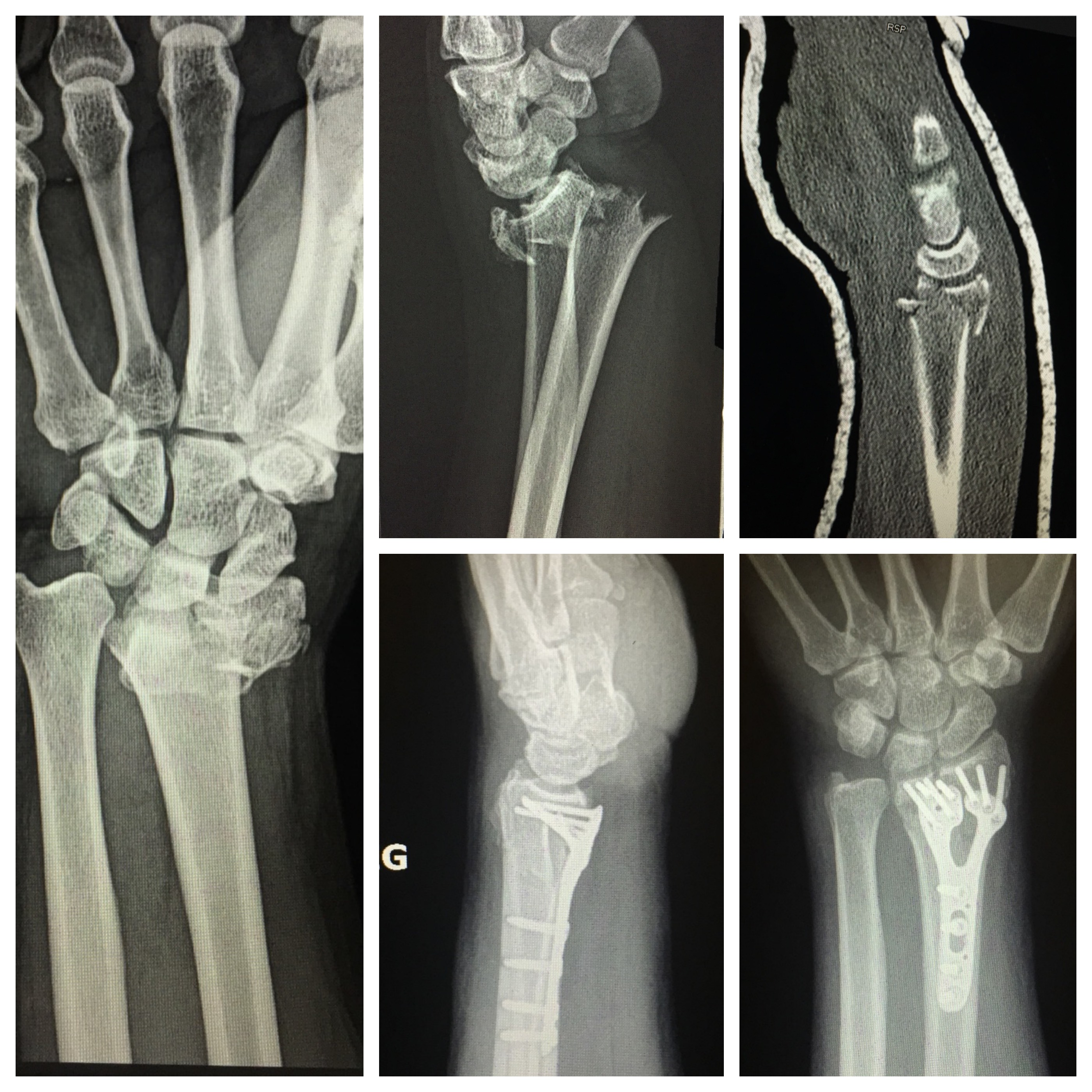
Case #2
The adult patient in the images below sustained an intra-articular distal radius fracture after a fall from height. CT scan was obtained for pre-operative planning showing the displaced joint surface. The patient underwent surgery, open reduction and internal fixation (ORIF) with plate and screws due to the severity of the injury.