As the weather gets nice, we see more pediatric wrist fracture injuries as kids are active, playing outside on trampolines, monkey bars, scooters, and bicycles.
Children are not just little adults. Kids have developing bodies which respond much differently to injuries than adults. Injuries to the bones and joints of pediatric patients take special orthopedic treatment to avoid problems with healing and growth.
Kids are different:
- Growth Plates: Children have growth plates near the end of the bones which allow the bones to lengthen and grow as the child ages. The growth plate is called the physis. In adults, the physis has closed, as the bones are no longer growing.
- Remodeling: Children have the ability to reshape their bones as they grow. In many cases, if a child has a crooked bone, it can be reshaped or remodeled straight as the child develops. If you have seen a crooked tree grow straight over time after being braced by a gardener, you might understand this concept. Adults do not have this ability.
- Bones are more flexible: Kids bones are more flexible and less brittle than adults. Because of this, the bones can bend or bow instead of breaking.
- Kids heal faster: For most children, the healing process is much quicker than in adults. This is important, because a delay in treatment can result in a quickly healed bone in a poor position.
- Ligaments are strong: In most cases, the ligaments in children are stronger than the bones. This means that a child is much more likely to break a bone than tear a ligament. This fact creates unique fractures patterns only seen in kids.
I tell parents that kids bounce back much faster than their parents. In most cases, children heal their bones quickly, they have less problems with swelling and stiffness, and they return to school and sports much sooner than most people expect.
On the other hand, problems can arise in kids which take special care and treatment. A growth plate injury can result in stunted growth and an imbalance in bone length. In the wrist, for example, if the distal radius physis is badly damaged and the radius bone stops growing, the ulna bone can keep growing and become much longer than the radius. This can cause wrist pain and limited range of motion later in life.
The amount of remodeling or reshaping of the bone is related to the child’s age and development. Young children have more potential to remodel the bone after a fracture. If the child is older and in adolescence, there is less potential for the bone to straighten out with time.
A broken wrist often involves the end of the radius bone, called the distal radius. There are several types of distal radius fracture:
- Buckle fracture: Buckle fractures are very common in children less than 10 years of age. These fractures result when the bone is compressed and raises a “buckle” or bump on one side of the bone without breaking the other side of the bone. These fractures do not need surgery. Most kids are treated with a cast for a few weeks and the long-term outcome is excellent.
- Salter-Harris fracture: These are fractures which involve the growth plate. Salter-Harris fractures are classified 1-5 depending on the location and severity of the fracture. Most pediatric S-H distal radius fractures are type 2, and these usually heal very well. Close evaluation of the growth plate is needed to rule out bone growth disturbances.
- Metaphysis fracture: Fractures in the metaphysis are common in children. This is the area of the bone which flares out near the wrist joint and is a common location for injury. Kids who have fractures which are well-aligned do not need surgery, and are usually treated with a few weeks of casting. Fractures which are crooked or shifted out of position are often treated with manipulation and casting without surgery. The manipulation procedure is often performed in the emergency room with sedation or the operating room with anesthesia. Sometimes surgery is needed to fix the fracture with temporary pins (closed reduction and percutaneous pinning).
- Forearm fractures: The radius and ulna bones can be broken within the shaft of the bones. This is called a both-bone forearm fracture. These fractures are usually displaced and angulated (separated and crooked) due to the trauma. Most pediatric both-bone forearm fractures can be treated with manipulation and casting without surgery. The manipulation procedure is often performed in the emergency room with sedation or the operating room with anesthesia. Sometimes surgery is needed to fix the fracture with plates and screws (open reduction and internal fixation) or rods within the hollow canal of the bone (intramedullary nailing).
How to improve healing. Make sure your child has good nutrition. Bones need calcium and protein to heal. This means dairy products such as milk, yogurt, cheese, ice cream, as well as beef, fish, chicken, pork, beans, and green vegetables. Getting outside in the sun helps with getting vitamin D, which is needed for healthy bones. While the fracture is healing, give it some rest and protect the area. What I tell kids is “keep your feet on the ground.” This means no bikes, scooters, monkey bars, trampolines, or climbing while the fracture is healing. For most pediatric distal radius fractures this is about 3 months of protection from repeat injury.
Case Example #1:
Below are x-rays of a young child who sustained an angulated, displaced both-bone forearm fracture. The patient underwent closed reduction and splinting in the emergency room on the night of the injury. The child was treated with an above-elbow cast for 3 weeks and a forearm cast for another 4 weeks. Callous is seen on the follow-up x-rays in the clinic 2 months after the injury.

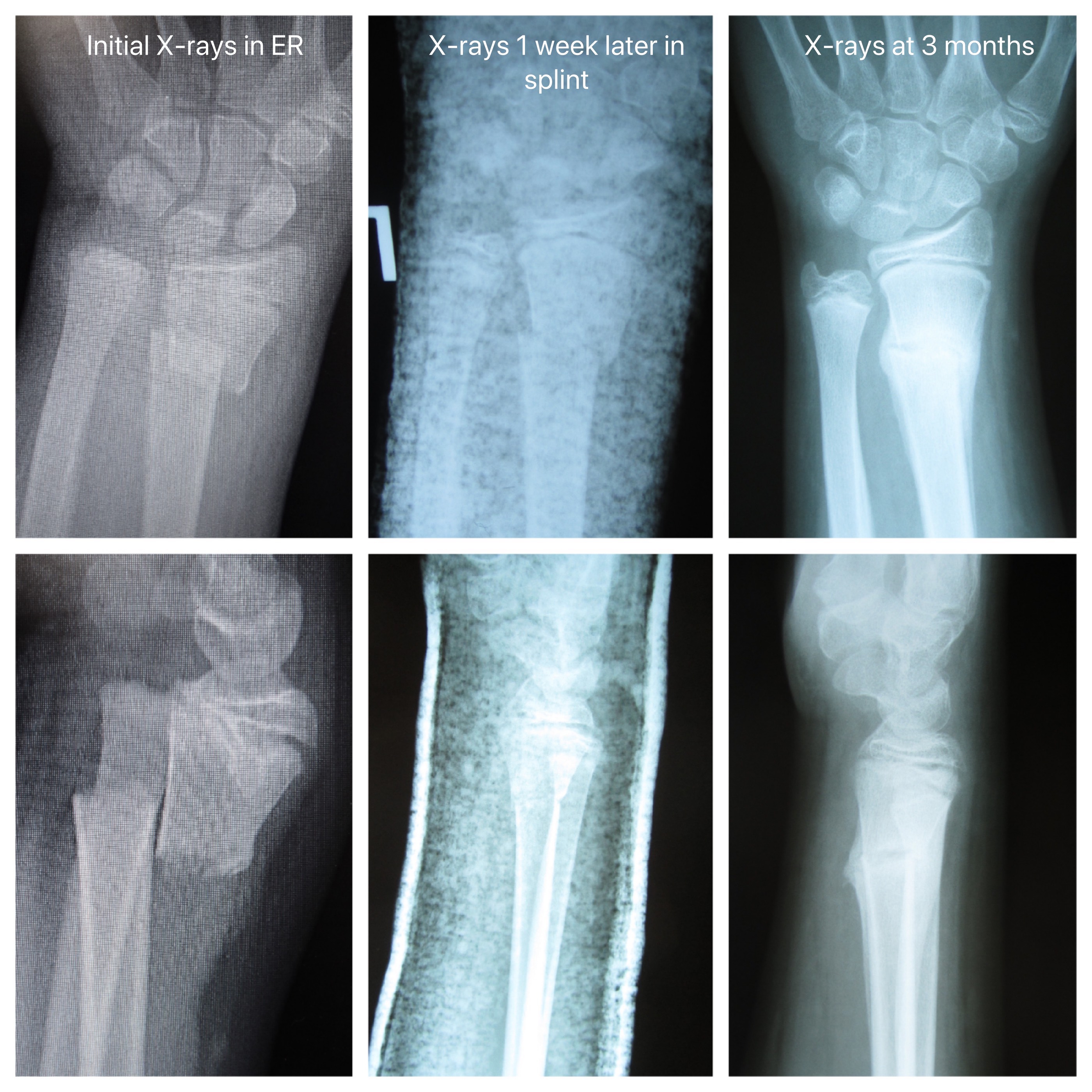
Case Example #2:
Below are x-rays of a young child with wrist fractures of the distal radius metaphysis and distal ulna. Significant fracture displacement is seen on the initial x-rays. The child underwent closed reduction in the emergency room with splinting. X-rays at follow-up in the office one week later show much improved alignment. The child was treated with 6 weeks of casting, and had a very good result. On the 3 month follow-up x-rays you can see the normal, extra bone formation at the fracture site, called callous.